When is Sciatica NOT a Sciatica?

Sciatica is a complaint that often does not respond to care, not because it is difficult to treat but more often because it is some other problem.
“My office specializes in treating chronic and difficult cases so I often see common conditions that have not been resolved even though the patient has seen multiple physicians. ” – Dr. Zodkoy, DC
 Sciatica is a specific diagnosis indicating pressure on the L 4 and L5 nerve roots that refers pain down the leg. Too often physicians and patients use Sciatica as a generalized term for leg radiculopathy pain which leads to inadequate care and years of pain. There are several other conditions that mimic and are often referred to as Sciatica but will not respond to the care used to treat sciatica.
Sciatica is a specific diagnosis indicating pressure on the L 4 and L5 nerve roots that refers pain down the leg. Too often physicians and patients use Sciatica as a generalized term for leg radiculopathy pain which leads to inadequate care and years of pain. There are several other conditions that mimic and are often referred to as Sciatica but will not respond to the care used to treat sciatica.>Piriformis Syndrome is the most common mimic of Sciatica. The Piriformis muscle starts on the anterior side of the low back and runs forward, inferior and lateral to the edge of the femur “hip bone’. This muscle is responsible for rotating your hip/leg out, like when you sit in a yoga position. The sciatic nerve runs adjacent to the Piriformis muscle which is why their symptoms often mimic each other. If this muscle goes into spasm a person may feel; back pain, hip pain, buttock pain, leg radiculopathy and have difficulty moving their back and leg. These are the same symptoms indicated in Sciatica, so how do you know the difference? Your doctor should be able to do an exam and pinpoint the main cause of your condition.
The simplest test is to palpate the L4 /L5 and the sciatic notch regions, the area which causes more pain is usually the primary issue, it is possible to have both conditions. The treatment for Piriformis Syndrome is focused on relaxing the muscle which include pelvic adjustments, trigger point therapy and modalities. The most effective treatment is Litecure Laser Therapy which can quickly penetrate deep into the muscle to relieve the spasm and reduce inflammation.
Iliotibial Band (ITB) Syndrome refers to a muscle that runs from your hip to below your knee, like the pathway that the Sciatic nerve follows. ITB syndrome is caused by the irritation and weakness of the Tensor Facia Lata (TFL)muscle but not a nerve. This condition is often caused by physical activity or shoes that cause your ankles to supinate (roll in).
The condition must always be ruled out before giving a diagnosis of Sciatica because it will not respond at all to sciatic treatment. Your doctor can diagnose this problem by testing the strength of the TFL and Popliteus muscles in your legs, weakness is a good indicator of this condition.
Palpation of the TFL muscle, sciatic notch and L4/L5 region is also done because ITB syndrome does not affect these areas. Correcting this condition requires finding the cause which may include a person’s gait or shows, strengthening the muscle and reducing inflammation in the area. I use Applied Kinesiology to evaluate my patient’s gait and shoes, kinesiology tape to stabilize and strengthen the muscle and the Litecure Laser to reduce inflammation.
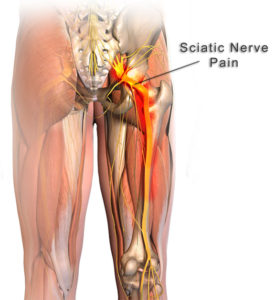
The final mimicking condition that needs to be evaluated when a person says they have Sciatic is an impinged Common Peroneal Nerve. The Sciatic nerve turns into the Common Peroneal nerve at the knee level (see Fig. 1). Impingement of he Common Peroneal nerve at the knee is a common cause of pain above and below the knee which is why it mimics sciatica.
Your doctor can diagnose the difference by palpating behind lateral part of the knee where the Common Peroneal begins, acute pain is an indicator that is a major issue. ITB syndrome and Common Peroneal nerve impingement often show up together because the Tensor Facia Lata muscle is major stabilizer of the Fibula bone which is adjacent to the Common Peroneal Nerve.
The treatment for this condition includes Applied Kinesiology to evaluate my patient’s gait and shoes, mobilization of the Fibula, kinesiology tape to stabilize the Fibula and the Litecure Laser to reduce inflammation.
Too often physicians are in a rush to properly evaluate the underlying cause of their patients’ pain and thus miss the true diagnosis, this is most apparent when it comes to Sciatic pain. If your Sciatic pain has not responded to treatment make sure your doctor is not treating a Sciatic mimic.